
What’s behind the Soaring Chronic Diseases?
Author: Jian Gao, PhD
Editor: Mr. Frederick Malphurs
September 9, 2023
Not Our Genes
Our genes have been made a scapegoat for the skyrocketing prevalence of chronic diseases. Given some are plagued with chronic disease while others are not even though they live in the same environment, and chronic diseases such as hypertension often run in families, the culprit must be the genes, right? Wrong. As intuitive as it is, the assertion that genetic factors are behind the soaring of chronic diseases is spurious – pure and simple.
Myriad chronic diseases such as obesity, diabetes, and heart disease have skyrocketed – they were rare 80 years ago even after age and life expectancy are considered. Have human genes changed? No. Even if the genes changed, they did so to make the diseases less likely, at least not more likely – the process and result of evolution.
You might wonder then, why some get sick while others do not? Well, that is because our genes differ from one person to another and thus the detoxification capacity varies. When the environment changes (e.g., more and more toxic chemicals), those with weaker detox genes (which, of course, run in families) and high exposure to toxins (e.g., those who rely on processed food loaded with harmful chemicals, or live close to toxic industrial sites) would not adapt well.
Do not blame your genes. Except for rare mutations (e.g., cystic fibrosis and sickle cell anemia, which have not increased in the last 80 years), there are no good or bad genes – genetic variations from person to person are normal and indispensable. Evolution works by natural selection – without variations, there would be no evolution because there would be no difference in genes to select from – humankind could be wiped out by a single virus or plague.
The soaring incidence of chronic diseases is clearly caused by the changing environment rather than genes simply because nothing else has changed much. And despite all the resources poured into genetic research and all the hype, no genes have been found to be the main driver of any common chronic diseases, which inflict unmeasurable suffering – obesity, diabetes, hypertension, heart disease, mental disorders including autism and dementia just to call out a few, in addition to the more than 100 autoimmune diseases.
Not to forget the emperor of all maladies: is cancer caused by bad or rogue genes? Thanks to the continued promulgation by the medical establishment, the so called “bad luck” theory is still metastasizing, which states two thirds of the cancers are due to random genetic mutations and thus not avoidable or preventable.1-5 The theory was created by two influential articles published in the prestigious journal Science in 2015 and 2017,6,7 which reached the conclusion based on a statistic, R-squared = 0.65, meaning 65% or two third of the cancers are explained by random mutations during normal stem cell divisions.
First, the notion that random mutations cause cancer does not even pass the laugh test. If the number of cell divisions and thus random errors were the culprit, there would be no elephants or blue whales – they have 100 and 2,000 times more cells and thus more random errors respectively than humans and yet rarely get cancer. Furthermore, the latest research published in the journal Nature indicates random mutations are not really random – organisms evolve to protect themselves and enhance survival rather than aimlessly drift.8
Even if cancers were caused by random mutations, an R-squared of 0.65 means 40% of the cancers are explained by random mutations, not 65% or two thirds. The exaggeration is due to the misconception of R-squared in statistics.
Even for the strongest cancer genes, BRAC1 and BRAC2, the risk of getting breast cancer was 24 percent before 1940 for the mutation carriers.9 Today, the risk is about 80 percent. And keep in mind, although one cancer case is too many, BRAC1 and BRAC2 only contribute about 3% of all breast cancer.
Studies on identical twins have clearly demonstrated genetic factors only play a minor role in cancer development. For instance, a large international study published in the New England Journal of Medicine, which analyzed 44,788 pairs of twins listed in the Swedish, Danish, and Finnish twin registries, has revealed the rates of cancer concordance in twins are generally below 0.1 – strongly suggesting less than 10% of the cancers are a result of genetic factors.10
Despite the cancer industry and the medical establishment wanting us to believe otherwise, genes are not the major driver behind the skyrocketing cancer incidence and other chronic diseases in the last 80 years. Genes are not our destiny.
Not Our Age
On the surface, data show a clear correlation between age and chronic diseases. As a result, the aging of the population is blamed for the soaring number of chronic diseases. It is true we are losing muscle and memory as we age, just as the law of gravity – nobody can escape. But except for wear and tear, there is little reason or scientific evidence to believe age by itself causes these common chronic diseases such as obesity, diabetes, autoimmune diseases, mental disorders, and cancer. Many may wonder then, why data show older people are more likely to have chronic diseases? The answer is simple – older people have accumulated more insults from environmental toxins and noxious psychological stress from adverse life events.
Furthermore, even from a pure data perspective, the rising prevalence of chronic disease has far outpaced the rate of aging. And most of the data showing the steep upward trends of chronic diseases are age-adjusted. In other words, even for people of the same age, the prevalence of chronic diseases is several-fold higher than 80 years ago.
Clearly, all the evidence leads to an inescapable conclusion: environmental chemicals rather age itself are the culprit behind the soaring chronic diseases – it is as simple and certain as 2 + 2 = 4. If you still do not believe it, just look at the incidence of autism – according to CDC, the incidence has increased 417% from 1 in 150 to 1 in 36 children in just 20 years from 2000 to 2020. Is it because of age?
And why are cancer victims getting younger and younger? For instance, the childhood cancer incidence rate (cases per 100,000 population) in Denmark jumped 75% from the 1930s to the 1990s. In the US, it increased by 36 percent in 13 years from 1980 to 1993. A recent study, which is published by researchers from Harvard University and widely covered by major news networks, shows the incidence of early-onset cancers like colorectal and 13 other types of cancers are rising rapidly in many countries including the US.11 The latest research published in 2023 by the BMJ (British Medical Journal) Oncology concluded “Global incidence of early-onset cancer increased by 79.1% and the number of early-onset cancer deaths increased by 27.7% between 1990 and 2019.”12
Clearly, age is not the driver behind cancer. On the contrary, age should be an anticancer factor – older cells are better trained in what they do and slow in dividing and growing.13
Rather than identifying and fixing the root causes, the medical establishment loves to find scapegoats – genes and aging, which are not avoidable, preventable, or curable – just swallow more pills.
Not Our Lifestyle Either
There is no doubt smoking, drinking, and sedentary lifestyle are detrimental to our health. However, for the last 80 years, fewer and fewer people are smoking, Gallup Polls reveal the trend of alcohol consumption has been flat since 1939, and studies have shown we are physically exercising more.14-17
The government agencies and health experts admonished us that fat was the cause of heart disease, so we laid off fat consumption. And then we are told sugar is the problem, and we followed their advice too. But more and more people have been getting sicker and sicker. Let alone other chronic diseases, even obesity went the opposite direction when compared with sugar consumption. Take Australia for example, from 1980 to 2003, sugar consumption per capita decreased by 23%, but the prevalence of obesity has increased 3-fold,18 which is widely referred to as the Australian Paradox. Following Australia, the US witnessed a similar pattern: from 2001 to 2018, added sugar intake decreased from 16.2 to 12.7% of calories,19 yet the obesity prevalence increased from 30.4% to 42.4%.20,21
There is no doubt too much sugar consumption is not healthy and there are still pockets of individuals eating too much sugar or refined carbs and not physically active enough, like smokers and drinkers. But given the opposite trend of sugar consumption compared to obesity prevalence, clearly sugar is not the chief culprit behind the obesity epidemic and other chronic maladies.
Another popular theory claims that consuming too many calories is behind the soaring prevalence of chronic diseases – excessive calories cause obesity which in turn induces other maladies including cancer. As convenient as it is, this theory does not hold water either. In fact, over the last decades, calorie intake has not increased. For instance, NHSNES (the National Health and Nutrition Examination Survey), arguably the most reliable data source on this topic, shows calorie intake has decreased from an average of 2,234 (kcal/day) in 1988 to 2,050 in 2016 in the US,22,23 while the prevalence of obesity and overweight took off during the same period.
It is true that the obesity rate and the prevalence of other chronic diseases have been in lockstep during the past 30-40 years, but more likely than not, both the obesity epidemic and other chronic diseases are driven by the changing environment rather than causal factors of each other.
No matter how you slice it, single-mindedly focusing sugar, calories, and lifestyle will not get us out of the health crisis.
Toxic Chemicals – The Greatest Threat to Our Health
With mathematical certainty, toxic chemicals in our food, water, air, personal products, and homes are collectively the main driver behind the soaring of chronic diseases in the last 80 years – there are no other factors that have the scope, the biological ‘know-how’, and the trend (production and use) parallel to the trend of chronic diseases.
The medical establishment and even well-intentioned scientists who are unfortunately reductionistic cannot wait to challenge this conclusion. Which chemicals and how? – they love to argue the findings are inconsistent. Of course, the results are inconsistent – focusing on the causal relationship between a single chemical (or maybe a couple of chemicals) and a disease will never attain consistent findings. There are thousands of toxic chemicals interacting with each other in our body along other risk factors such as stress, and most likely the total toxic burden of our body makes the difference (the same enzymes in our body are needed for detoxification). Yet, the medical establishment and unfortunately the reductionists continue to maintain a single-minded focus on the relationship between one chemical (e.g., glyphosate or Roundup) and one disease (e.g., cancer).
Chemicals in Our Food
Our food, including grains, vegetables, fruit, meat, and dairy, is laden with insecticides, herbicides, fungicides, and other chemicals which are known to be carcinogenic besides causing other maladies. Particularly, animal products are loaded with antibiotics, growth hormones, and other novel chemicals designed to increase production and profit. For example, it only takes about six months to grow pigs from birth to slaughter, and 6-8 weeks to grow chickens. Normal cows can only produce a gallon of milk a day, but the use of chemicals increases production to six gallons a day.
As if these poisons were not bad enough, over 10,000 chemicals in at least 20 categories are added into our food by manufacturers for different purposes such as coloring or increasing shelf life.24,25
Although most of these additives are safe, the health effects of many of them are unknown, and many are known to be carcinogenic. For instance, the artificial sweetener saccharin, which has been shown to cause cancer in animals, is still used in food and soft drinks.26,27 Nitrates and nitrites are two known cancer-making compounds (mainly through reacting with other chemicals), but are still used to preserve processed meats.28,29 Potassium bromate is a possible human carcinogen because it has been shown to cause kidney, thyroid, and gastrointestinal cancer in animals. Although potassium bromate has been banned in Europe and many other countries around the world, it is still legally and widely used in many baked goods in the US to strengthen dough and allow it to rise higher, as reported in CBS Evening News on January 20, 2023.
Other similar toxic additives are azodicarbonamide (whitening flour), ractopamine (a popular feed additive for pigs and beef cattle to grow more muscle mass), titanium dioxide (makes food like candy, coffee creamer, baking, and cake decorations more visually appealing), BVO (brominated vegetable oil used to keep citrus flavoring from separating out in sodas and other beverages), olestra (a fat substitute that adds no calories to products), propylparaben (a food preservative), and the list goes on.
The unknowns are even more unsettling – the long-term health effect of countless food additives is unknown thanks to the GRAS (Generally Recognized as Safe) loophole in a 65-year-old law (the Food Additive Amendment signed into law in 1958) allowing food manufacturers to circumvent the approval process by FDA. As long as a food company deems an additive GRAS, no report to FDA is required.24,25
In addition to the chemicals directly added to food, dangerous chemicals in food-packaging materials also leach into our food. Take for example, two known carcinogens, vinyl chloride and acrylonitrile, are still used in making food containers.27 And food manufacturers clean their equipment with hazardous chemicals which gets into our food too, which was exposed by the child labor scandal in the meat processing industry early in 2023.
Additionally, we also swallow tons of prescription drugs such as antidepressants and over the counter pills like ibuprofen – they are chemicals and often do more harm than good. In particular, chemotherapies themselves are in fact potentially cancer makers.
Chemicals in Drinking Water
If you think our drinking water is pure and wholesome, you are mistaken. First, where do all the runoff fertilizer and pesticides from residential and agricultural use go? Second, where did/do all the chemicals discharged from all the manufacturers go? Third, where do all the chemicals ending up in landfills go? Fourth, where do all prescription and over the counter drugs either discarded or metabolized go? Fifth, what contaminants are tested or not tested at your municipal water plant? Sixth, do you know most of the pipes carrying water from the treatment plant to your home contain lead? Finally, are the chemicals such as chlorine used by water treatment plants for disinfection safe?
As to the first question, here is what USGS (United States Geological Survey), a government agency focusing on biology, geography, geology, and hydrology of the landscape, has to say, “Considerable increases in fertilizer and pesticide use began in the 1960s. In 2010, about 11 billion kilograms of nitrogen fertilizer and 300 million kilograms of pesticides were used annually to enhance crop production or control pests… Fertilizers and pesticides don’t remain stationary on the landscape where they are applied; runoff and infiltration transport these contaminants into local streams, rivers, and groundwater.”30
Nobody knows how much or how many synthetic chemicals producers and users have dumped into the environment since the 1940s. Among all the manmade chemicals discharged into the environment, the “forever chemicals” PFASs (per- and polyfluorinated compounds), especially its two family members PFOA (perfluorooctanoic acid) and PFOS (perfluorooctane sulfonate), have been thrust into the spotlight recently due to numerous incidents of widespread contamination and mounting evidence of toxicity.
PFAS, a class of over 4,000 different manmade chemicals including PFOA and PFOS, is truly ubiquitous – you can find them in hundreds of common household items such as furniture and carpet, water-repellent clothes, cosmetics, cleaning products, fast food wrappers, nonstick pans, paints, firefighting foams – they are detectable in the blood of 98 percent of us.
Of course, they are in our drinking water. In a recent report, EWG (Environment Working Group) stated, “Based on our tests and new academic research that found PFAS widespread in rainwater, EWG scientists now believe PFAS is likely detectable in all major water supplies in the U.S., almost certainly in all that use surface water… Of tap water samples from 44 places in 31 states and the District of Columbia, only one location had no detectable PFAS, and only two other locations had PFAS below the level that independent studies show pose risks to human health.”31
“I think it’s one of the biggest threats in drinking water that people don’t have a complete understanding of, and it’s been around for decades,” says David Andrews, PhD, a senior scientist at the EWG who was involved with the report.
In fact, the number of communities confirmed to be heavily contaminated with PFAS in the US continues to grow at an alarming rate – as of June 2022, 2,858 locations in 50 states and two territories are known to be contaminated.32
One of these locations is close to home – Hoosick Falls, a small town near Albany, New York, where I have lived and worked for 30 years. Despite the danger, nobody knew about the contamination for decades until Hoosick Fall’s resident Michael Hickey launched his own investigation into the town’s water supply since he was concerned about the high rate of cancer in the community. His father, John Hickey, died of kidney cancer in 2013. His father worked for decades at the Saint-Gobain Performance Plastics plant using PFOA, a member of PFAS, to make Teflon for non-stick cooking ware.
In 2014, after searching the connection between PFOA and cancer he took samples from the town water and sent them to a lab for testing on his own dime. The results showed high levels of PFOA and caught the attention of the New York State Department of Health which ran further tests revealing PFOA levels as high as 600 ppt (parts per trillion) in sharp contrast to the EPA health advisory level for PFOA and PFOS at 70 ppt individually or combined.33 And the tests also revealed the PFOA contamination reached 18,000 ppt in the groundwater near Saint Gobain plant and 21,000 ppt at a nearby dump site.
At long last, EPA has started to realize the gravity of the PFAS problem which extends far beyond the heavily contaminated sites. On March 14, 2023, for the first time, EPA announced the proposed National Primary Drinking Water Regulation (NPDWR) for six PFAS including perfluorooctanoic acid (PFOA), perfluorooctane sulfonic acid (PFOS), perfluorononanoic acid (PFNA), hexafluoropropylene oxide dimer acid (HFPO-DA, commonly known as GenX Chemicals), perfluorohexane sulfonic acid (PFHxS), and perfluorobutane sulfonic acid (PFBS). In the proposal, the limit set for PFOA and PFOS is 4 ppt, which is dramatically lower compared to the EPA health advisories recommended level of 70 ppt in 2016. Another four PFAS (PFBS, PFNA, PFHxS, and GenX) will be regulated as a mixture using a “hazard index.”
The proposed rule is now open to a period of public comments. EPA will take those comments into consideration for the final decision on the rule. “We anticipate that when fully implemented, this rule will prevent thousands of deaths and reduce tens of thousands of serious PFAS related illnesses,” stated EPA Administrator Michael Regan at a news conference announcing the proposal on March 14, 2023, in Wilmington, North Carolina. This sounds great – finally EPA is taking action. On the other hand, EPA has just told us these chemicals have been killing thousands and sickening more but did nothing to stop it for decades.
A reasonable question to ask is, why did EPA drag its feet for so long while people are getting sick and dying? It is never too late, but it is still too little.
In addition to the chemicals for industrial use, chemicals used in homes are a problem too. Let alone the poisonous pesticides and cleaning products we use every day, the ingredients of all the common medications can also be detected in drinking water, which means the chemicals in the landfill (pills thrown away) and sewage systems (pills taken and metabolized) end up in the drinking water system.
The worst part is we don’t know what we don’t know. Municipal drinking water treatment plants don’t test for these chemicals because they don’t know what to test for.
Municipal drinking water treatment plants indeed test for some heavy metals such as arsenic and lead. But the lead levels at homes could be very different from the levels at the water treatment plants because lead in the aged water pipes underground can leach out. That was the cause of the Flint water crisis in Michigan. Lead contamination is not unique to Flint – before lead pipes bringing water into homes were banned in 1986 nationwide, most water pipes underground were made of lead or at least contained lead (lead pipes were used because they are stable, flexible, and rarely leak – they can reshape and adapt as the ground moves). Thank heavens, the lead problem will likely be gone as the $1 trillion Infrastructure Investment and Jobs Act is implemented. But other problems remain.
An even more insidious problem is the collateral damage from water disinfection using chlorine. The implementation of drinking water disinfection and filtration is considered as one of the most important public health advances of the last century, which has effectively eliminated waterborne infectious diseases and poisoning. “But the use of chlorine has a dark side: In addition to inactivating waterborne pathogens, chlorine reacts with natural organic matter to produce a variety of toxic disinfection by-products (DBPs),” reported in the prestigious journal Science.34 Studies found an increased risk of bladder cancer after life-long ingestion of chlorinated drinking water.35-38 EPA has accepted exposure to DBPs increased 2-17% of the bladder cancer cases.39
In addition to cancer, DBPs are also linked to other health problems such as birth defects.40-42 The health hazards of DBPs have since been well recognized worldwide. Unfortunately, the full scope of health problems caused by DBPs is yet to be uncovered. Scientists don’t even know how many DBPs are in treated water – at least half of the DBPs are unknown because chlorine is chemically so reactive it reacts with almost everything.38 Among over 600 DBPs that has been identified and reported,37 currently EPA only regulates chlorite, bromate, THMs (trihalomethanes), and HAAs (haloacetic acids).
Chemicals in the Air
Overall, outdoor air quality in north America has been getting better for the last decades. However, indoor air quality has been heading in the other direction – it has increasingly become a threat to our health. Residential houses have become more and more airtight for energy efficiency with very limited mechanical ventilation. Meanwhile, more and more synthetic materials have been getting into our homes, from building materials such as compressed wood boards and fire retardants (in carpets and padding) to household products such as cosmetics and cleaning products. In fact, it is hard to think of anything in our homes which is not synthetic or semisynthetic. All these chemicals and plastics emit toxic gases or particles into the air circulating inside our homes.
Indoor air can be very deceptive even if it is heavily polluted – colorless, smogless, and often odorless. One of the lurking dangers in our home is VOCs (volatile organic compounds) which are harmful chemicals emitted as gases from synthetic materials. Here’s a statement from the EPA (Environmental Protection Agency): “Concentrations of many VOCs are consistently higher indoors (up to ten times higher) than outdoors. VOCs are emitted by a wide array of products numbering in the thousands. Examples include paints and lacquers, paint strippers, cleaning supplies, pesticides, building materials, and furnishings, office equipment such as copiers and printers, correction fluid and carbonless copy paper, graphics and craft materials including glues and adhesives, permanent markers, and photographic solutions.”43
A 2023 study published in Environmental Science & Technology revealed over 5,000 tons of VOC were emitted from consumer products in 2020 in California alone.44
It’s well-known that VOCs cause respiratory disorders such as asthma, bronchitis and allergies. But that is only the tip of the iceberg. The real danger is their invisible actions – they silently, stealthily, and slowly damage every organ and system of our body and contribute to almost every disease. Some of them are known to be carcinogenic. For example, formaldehyde causes cancer,45-47 which is widely used in countless products such as plywood, particle board, and oriented strand board (OSB, engineered wood like particle board) used in building homes (sheathing in walls, flooring, and roof decking) and making furniture. It’s also found in many consumer products like cosmetics, dish soaps, medicines, and leather. And it’s in the fabric of our clothing to give the permanent-press effect, increase stain resistance, and improve colorfastness.
Ironically, among all the manmade products in our homes, cleaning products including air freshers are supposed to keep us healthy, but their danger is often overlooked. Here is what American Lung Association tells us: “Many cleaning supplies or household products can irritate the eyes or throat, or cause headaches and other health problems, including cancer. Some products release dangerous chemicals, including volatile organic compounds (VOCs). Other harmful ingredients include ammonia and bleach.”48 Worse still, these chemicals released from cleaning supplies can react with other pollutants in the air to form new toxins which trigger illnesses including cancer.49-53
While manmade chemicals in the air endanger our health, not all natural substances are benign either. Asbestos is one of them. Asbestos is a group of six naturally occurring fiber-like minerals which are soft, flexible, and heat-resistant. Because of its desirable properties, asbestos was once widely used in insulation and cement as well as consumer products such as cloth, paper, and plastics. Thanks to research revealing exposure to asbestos causes cancers and other diseases, the use of asbestos has become highly regulated.54
Nevertheless, according to the National Cancer Institute, up to 5,000 consumer products contained asbestos, many of which are still in use. Unlike many other chemicals, asbestos is stable and does not emit into the air by itself. But it can easily become airborne if old materials containing asbestos are disturbed. Asbestos is very nasty – once inhaled or ingested, the mineral fibers become permanently trapped in the body and cause real damage to the lung and other organs. Anyone living in houses built before the 1980s or handling old household items should be mindful about the danger posed by asbestos.
Asbestos has been banned in 55 countries worldwide, but not in the US. Like many other toxic chemicals, manufacturers put up a ferocious fight to stay in business. These companies made enormous profits by selling asbestos as insulation to shipbuilders during World War II and further expanded their business during the postwar building boom. They fought in courts with the help of unscrupulous researchers like J.C. Wagner who first identified the danger of asbestos and then changed his position to defend the asbestos companies in courts. Later it was revealed he was paid by these asbestos manufacturers.55 That is why asbestos was not phased out until the 1980s and is still not banned in America.
Poor air quality is not just a problem in homes. It can be bad in office buildings too depending on the materials used in construction and how many synthetic products are placed for use in the buildings.56 In particular, thousands of indoor sports fields and playgrounds in schools and gyms around the country are covered with crumb rubber from recycled tires and plastics containing VOCs like toluene, polycyclic aromatic hydrocarbons, and other dangerous chemicals like phenylmercuric acetate that may be linked to cancer. These rubber floors also contain heavy metals like lead and mercury.
As the floors age and wear down, toxic particles are released into the air and become health hazards. This lurking danger came to the national spotlight after a 36-year-old PE teacher in New Jersey was diagnosed with rare kidney cancer in 2013.57
Finally, our skin, the largest organ of our body, is ‘breathing’ too. Poisonous chemicals in beauty products and sunscreens do get under our skin – they travel deep into our body and poison every tissue and organ and induce cancer.58 “Since 2009, 595 cosmetics manufacturers have reported using 88 toxic chemicals in more than 73,000 products which have been linked to cancer, birth defects or reproductive harm.”59
Among the beauty products, hair treatment products are among the worst. Two recent large studies funded by the NIH have found hair straighteners and permanent dye greatly increase the risk of uterine and breast cancer.60,61
* * *
Taken together, toxic chemicals are ubiquitous and some of them are worse than others, but separating their individual ill effects is all but impossible. Nevertheless, burying our heads in the sand because the findings are ‘inconsistent’ is deadly foolish. Today, it is as certain as 2 +2 = 4 that toxic chemicals in totality are our greatest health foe (read chapter 2, Road to Health, for more detailed discussion).
Psychological Stress – A Health Killer
Protracted psychological stress does more harm to our health than almost anything else. However, stress should not be blamed for the epic increase of chronic disease incidence for the last 80 years. Stress has been with us for millions of years – extreme weather, famine, epidemics, flesh-eating animals, wars, and loss of loved ones, just to name a few, all create stress. At the population level, there is no evidence the stress level has increased over the last 80 years; on the contrary, existing evidence shows it has decreased somewhat.62
Nevertheless, chronic stress is a real health killer – our world was not disease free 80 years ago – stress has been a killer for millions of years although we have only started to understand its mechanisms in the last several decades. Literally, chronic stress interrupts every system and function in our body, and we feel it. For instance, when stressed out, our brain does not react rationally (nervous system), our heart races and blood pressure rises (cardiovascular and endocrine systems), our gut reacts negatively (digestive system), we are more prone to infections (immune system).
The greater danger is what we do not readily feel. For instance, stress induces dysbiosis (overgrowth of pathogenic bacteria in the gut) and disrupts intestinal and blood-brain barriers;63-65 more potently, stress alters gene expression,66-69 the conductor of our body’s orchestra. All these disruptions lead to all kinds of chronic diseases including cancer.70-76
Although stress cannot be blamed for the soaring prevalence of chronic diseases in the past 80 years, at the personal level, it is imperative to avoid and manage stress – we all experience or see most disease onsets happen under some kind of stress. Our body is overburdened with manmade toxic chemicals, and very often stress comes as the last straw breaking the camel’s back – the compounding effect of environmental chemicals and stress constitutes real danger to our health.
Other Factors
Toxic chemicals and stress are grizzly bears in the living room threatening our lives. However, smaller creatures like raccoons and even rats can cause real damage too if we turn a blind eye to them. Malnutrition is one of these things that can trip us.
Of course, in north America and many other parts of the world, deficiency in macronutrients (fat, protein and carbohydrate) is a thing of the far past. But the status of micronutrition (vitamins, minerals, and polyphenols from plants) is a different story. Despite fresh produce all year around in sparkling supermarkets and grocery stores illuminated with bright LED lights, not many people eat enough variety and quantity of fresh vegetables and fruits rich in minerals; instead, we rely too much on fast and processed food. In a 2017 press release, the CDC reported “Only 1 in 10 Adults Get Enough Fruits or Vegetables.”77
And the problem is compounded by the decline of micronutrients in vegetables, fruits, and grains – soil has been depleted of micronutrients due to intensive farming with chemical fertilizers.78-80 For instance, a recent study shows a 49.1% decrease of copper, 50.2% of iron, 51.7% of sodium, and 9.7% of magnesium in fruit and vegetables in the UK from 1940 to 2019.78
Consequently, the micronutrition status is troublesome. For instance, a US national survey (NHANES 2007-2010, which surveyed 16,444 individuals 4 years and older) revealed a high prevalence of inadequacies for multiple micronutrients.81 In particular, 94.3% of the population do not meet the daily requirement for vitamin D, 88.5% for vitamin E, 52.2% for magnesium, 44.1% for calcium, 43.0% for vitamin A, and 38.9% for vitamin C.
There are 17 identified essential minerals the human body can’t synthesize and must have: calcium, chloride, magnesium, phosphorus, potassium, sodium, sulfur, chromium, copper, cobalt, fluoride, iron, iodine, manganese, molybdenum, selenium, and zinc. Deficiency in any one of them will do harm to our health.
Let alone other chronic diseases,82 studies have shown a deficiency in micronutrients, such as vitamins B6, B9 (folic acid), B12, vitamin C, vitamin D, selenium, and zinc, increases the risk of cancer and mortality.83-89 This is in part because many micronutrients are cofactors for enzymes participating in detoxification,90 and micronutrient deficiency can also cause DNA damage (chromosomal breaks).91,92
In essence, micronutrient deficiency affects every function of our body. Yet, we collectively pay too little attention to it. Do you know your micronutrient status? Are you sure you are not deficient in any of them? Among all the micronutrients, vitamin D deserves special attention – deficiency and insufficiency are still widespread because about 90% of vitamin D we need is from the Sun while only about 10% is from food no matter how well you eat. Nowadays, few of us get enough sun exposure, and even in the sun, too many of us are covered with sunscreen which prevents the skin from making vitamin D.
The importance of vitamin D can be seen from the fact that every single cell in our body has Vitamin D receptors. Literally, vitamin D deficiency contributes to every single disease inflicted on humanity. Vitamin D deficiency or insufficiency is easy to fix – have your doctor test for it and bring it to the optimal level by either increasing sun exposure properly or taking supplements.
The Big Picture
Do not blame the genes – collectively, they have not changed in the last 80 years. And they became the victims of the changing environment too. There is no reason to believe age itself would bring on chronic diseases. And chronic diseases including cancer are increasingly hitting the younger generation including children. Do not use lifestyle as smokescreen. Yes, we can do better. But for the last 80 years, especially the last 30, by and large, we have been moving in the direction of healthier lifestyles, yet the prevalence of chronic diseases has been getting higher and higher.
Yes, countless risk factors can induce or contribute to chronic diseases. But for the last 80 years, nothing else has changed much except for the environment being soaked with more and more manmade chemicals. Is it not 2 + 2 = 4?
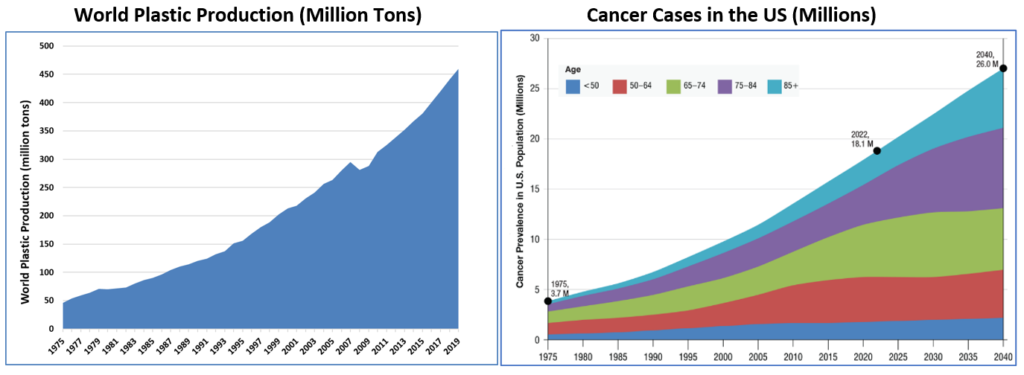

Data Sources: Top Left: Our World in Data; Top Right: National Cancer Institute (NCI); Bottom: 4 of the 21 graphs from a 2014 study.
Take Care of Yourself and Loved Ones
At the individual level, the root causes for the same disorder can be different from one person to the next. For instance, depression can be brought on by stress, neural toxins produced by pathogenic bacteria in the gut, heavy metals like lead, manmade chemicals like PCBs and pesticides, vitamin D and/or B deficiency, or any combination of these risk factors. No matter how complex the root causes are, they belong to these four categories: mind (stress), gut (intestinal permeability, and dysbiosis), environment (toxic chemicals, food sensitivity, and infections), and micronutrient deficiency. Of course, a proper lifestyle is a given. Mounting evidence has clearly shown most if not all chronic disease can be reversed once the root causes are removed. If your rifle cannot hit the target, bring your shotgun out – you only have four things to shoot.
About the Author and Editor: Jian Gao, PhD, is a healthcare analyst/researcher for the last 25 years who devoted his analytical knowledge and skills to understanding health sciences and clinical evidence. Mr. Frederick Malphurs is a retired senior healthcare executive in charge of multiple hospitals for decades who dedicated his entire 37 years’ career to improving patient care. Neither of us takes pleasure in criticizing any individuals, groups, or organizations for the failed state of healthcare, but we share a common passion – to reduce unnecessary sufferings inflicted by the so-called chronic or incurable diseases on patients and their loved ones by analyzing and sharing information on root causes, effective treatments, and prevention.
Disclaimer: This article and any contents on this website are informational or educational only and should by no means be considered as a substitute for the advice of a qualified medical professional. It is the patients and caregivers’ solemn responsibility to work with qualified professionals to develop the best treatment plan. The author and editor assume no liability of any outcomes from any treatments or interventions.
References
- Grady D. Cancer’s Random Assault. The New York Times. January 5, 2015. https://www.nytimes.com/2015/01/06/health/cancers-random-assault.html#:~:text=It%20may%20sound%20flippant%20to,happen%20when%20healthy%20cells%20divide.
- Healy M. ‘Bad luck’ with random DNA errors is responsible for two-thirds of cancer mutations, study says. Los Angeles Times. March 23, 2017. https://www.latimes.com/science/sciencenow/la-sci-sn-cancer-bad-luck-20170323-story.html.
- Wu S, Zhu W, Thompson P, Hannun YA. Evaluating intrinsic and non-intrinsic cancer risk factors. Nat Commun. 2018 Aug 28;9(1):3490. doi: 10.1038/s41467-018-05467-z. PMID: 30154431; PMCID: PMC6113228.
- Belizário JE. Cancer Risks Linked to the Bad Luck Hypothesis and Epigenomic Mutational Signatures. Epigenomes. 2018; 2(3):13. https://doi.org/10.3390/epigenomes2030013.
- Goldhaber S. The Randomness of Life: Bad Luck Cancers. American Council on Science and Health. June 24, 2021. https://www.acsh.org/news/2021/06/24/randomness-life-bad-luck-cancers-15629.
- Tomasetti C, Vogelstein B. Cancer etiology. Variation in cancer risk among tissues can be explained by the number of stem cell divisions. Science. 2015 Jan 2;347(6217):78-81.
- Tomasetti C, Li L, Vogelstein B. Stem cell divisions, somatic mutations, cancer etiology, and cancer prevention. Science. 2017 Mar 24;355(6331):1330-1334.
- Monroe JG, Srikant T, Carbonell-Bejerano P, et al. Mutation bias reflects natural selection in Arabidopsis thaliana. Nature. 2022 Feb;602(7895):101-105.
- King MC, Marks JH, Mandell JB; New York Breast Cancer Study Group. Breast and ovarian cancer risks due to inherited mutations in BRCA1 and BRCA2. Science. 2003 Oct 24;302(5645):643-6. doi: 10.1126/science.1088759. PMID: 14576434.
- Lichtenstein P, Holm NV, Verkasalo PK, et al. Environmental and heritable factors in the causation of cancer–analyses of cohorts of twins from Sweden, Denmark, and Finland. N Engl J Med. 2000 Jul 13;343(2):78-85.
- Ugai T, Sasamoto N, Lee HY, et al. Is early-onset cancer an emerging global epidemic? Current evidence and future implications. Nat Rev Clin Oncol. 2022 Oct;19(10):656-673. doi: 10.1038/s41571-022-00672-8.
- Zhao J, Xu L, Sun J, et alGlobal trends in incidence, death, burden and risk factors of early-onset cancer from 1990 to 2019BMJ Oncology 2023;2:e000049. doi: 10.1136/bmjonc-2023-000049
- Wyld L, Bellantuono I, Tchkonia T, et al. Senescence and Cancer: A Review of Clinical Implications of Senescence and Senotherapies. Cancers (Basel). 2020 Jul 31;12(8):2134. doi: 10.3390/cancers12082134.
- Whitfield GP, Hyde ET, Carlson SA. Participation in Leisure-Time Aerobic Physical Activity Among Adults, National Health Interview Survey, 1998-2018. J Phys Act Health. 2021 Aug 1;18(S1):S25-S36. doi: 10.1123/jpah.2021-0014. PMID: 34465654.
- Morseth B, Hopstock LA. Time trends in physical activity in the Tromsø study: An update. PLoS One. 2020 Apr 14;15(4):e0231581. doi: 10.1371/journal.pone.0231581. Erratum in: PLoS One. 2020 Nov 20;15(11):e0242998. PMID: 32287319; PMCID: PMC7156055.
- Booth VM, Rowlands AV, Dollman J. Physical activity temporal trends among children and adolescents. J Sci Med Sport. 2015 Jul;18(4):418-25. doi: 10.1016/j.jsams.2014.06.002. Epub 2014 Jun 12. PMID: 25041963.
- Knuth AG, Hallal PC. Temporal trends in physical activity: a systematic review. J Phys Act Health. 2009 Sep;6(5):548-59. doi: 10.1123/jpah.6.5.548. PMID: 19953831.
- Barclay AW, Brand-Miller J. The Australian paradox: a substantial decline in sugars intake over the same timeframe that overweight and obesity have increased. Nutrients. 2011 Apr;3(4):491-504. doi: 10.3390/nu3040491. Epub 2011 Apr 20. Erratum in: Nutrients. 2011 Aug;3(8):734. Erratum in: Nutrients. 2014;6(2):663-4. PMID: 22254107; PMCID: PMC3257688.
- DiFrancesco L, Fulgoni VL 3rd, Gaine PC, Scott MO, Ricciuto L. Trends in added sugars intake and sources among U.S. adults using the National Health and Nutrition Examination Survey (NHANES) 2001-2018. Front Nutr. 2022 Aug 18;9:897952. doi: 10.3389/fnut.2022.897952. PMID: 36061886; PMCID: PMC9434277.
- Hedley AA, Ogden CL, Johnson CL, Carroll MD, Curtin LR, Flegal KM. Prevalence of overweight and obesity among US children, adolescents, and adults, 1999-2002. JAMA. 2004 Jun 16;291(23):2847-50. doi: 10.1001/jama.291.23.2847. PMID: 15199035.
- Hales CM, Carroll MD, Fryar CD, Ogden CL. Prevalence of obesity and severe obesity among adults: United States, 2017–2018. NCHS Data Brief, no 360. Hyattsville, MD: National Center for Health Statistics. 2020.
- Ford ES, Dietz WH. Trends in energy intake among adults in the United States: findings from NHANES. Am J Clin Nutr. 2013 Apr;97(4):848-53.
- Marriott BP, Hunt KJ, Malek AM, Newman JC. Trends in Intake of Energy and Total Sugar from Sugar-Sweetened Beverages in the United States among Children and Adults, NHANES 2003-2016. Nutrients. 2019 Aug 25;11(9):2004. doi: 10.3390/nu11092004.
- Pressman P, Clemens R, Hayes W, Reddy C. Food additive safety: A review of toxicologic and regulatory issues. Toxicology Research and Application. 2017; Volume 1:1-22.
- Maffini MV, Neltner TG, Vogel S. We are what we eat: Regulatory gaps in the United States that put our health at risk. PLoS Biol. 2017 Dec 20;15(12):e2003578. doi: 10.1371/journal.pbio.2003578. eCollection 2017 Dec.
- National Cancer Institute (NCI). Artificial Sweeteners and Cancer: https://www.cancer.gov/about-cancer/causes-prevention/risk/diet/artificial-sweeteners-fact-sheet.
- National Research Council; Division on Earth and Life Studies; Commission on Life Sciences; Committee on Diet, Nutrition, and Cancer. https://nap.nationalacademies.org/catalog/381/diet-nutrition-and-cancer-directions-for-research.
- Chazelas E, Pierre F, Druesne-Pecollo N, et al. Nitrites and nitrates from food additives and natural sources and cancer risk: results from the NutriNet-Santé cohort. Int J Epidemiol. 2022 Aug 10;51(4):1106-1119.
- Grosse Y, Baan R, Straif K, et al; WHO International Agency for Research on Cancer Monograph Working Group. Carcinogenicity of nitrate, nitrite, and cyanobacterial peptide toxins. Lancet Oncol. 2006 Aug;7(8):628-9. doi: 10.1016/s1470-2045(06)70789-6.
- Agricultural Contaminants. https://www.usgs.gov/mission-areas/water-resources/science/agricultural-contaminants?qt-science_center_objects=0#qt-science_center_objects
- PFAS Contamination of Drinking Water Far More Prevalent Than Previously Reported. https://www.ewg.org/research/national-pfas-testing/
- PFAS Contamination in the U.S. (June 8, 2022) https://www.ewg.org/interactive-maps/pfas_contamination/
- FACT SHEET PFOA & PFOS Drinking Water Health Advisories https://www.epa.gov/sites/production/files/2016-06/documents/drinkingwaterhealthadvisories_pfoa_pfos_updated_5.31.16.pdf
- Sedlak DL, von Gunten U. Science. Chemistry. The chlorine dilemma. 2011 Jan 7;331(6013):42-3.
- Hrudey SE, Fawell J. 40 years on: what do we know about drinking water disinfection by-products (DBPs) and human health? Water Sci. Technol.: Water Supply. 2015, 15(4), 667-674.
- Cantor KP, Villanueva CM, Silverman DT, et al. Polymorphisms in GSTT1, GSTZ1, and CYP2E1, disinfection by-products, and risk of bladder cancer in Spain. Environ Health Perspect. 2010 Nov;118(11):1545-50.
- Hrudey SE. Chlorination disinfection by-products, public health risk tradeoffs and me. Water Res. 2009;43(8):2057-2092.
- Villanueva CM, Cantor KP, Cordier S, et al. Disinfection byproducts and bladder cancer – A pooled analysis, Epidemiology. 2004;15(3):357-367.
- Odom R, Regli S, Messner M, et al. Benefit-cost analysis of the stage 1D/DBP rule, J. – Am. Water Works Assoc.1999;91(4):137-147.
- Hwang BF, Jaakkola JJ, Guo HR. Water disinfection by-products and the risk of specific birth defects: a population-based cross-sectional study in Taiwan. Environ Health. 2008 Jun 2;7:23. doi: 10.1186/1476-069X-7-23.
- Hattersley JG. The negative health effects of chlorine. Journal of Orthomolecular Medicine. 2000;15(2):89-95.
- Zeighami E, Watson A, Craun G. Chlorination. water hardness and serum cholesterol in forty-six Wisconsin communities. Int J Epidemiol. 1990;19 (1):49-58.
- https://www.epa.gov/indoor-air-quality-iaq/what-are-volatile-organic-compounds-vocs
- Knox KE, Dodson RE, Rudel RA, Polsky C, Schwarzman MR. Identifying Toxic Consumer Products: A Novel Data Set Reveals Air Emissions of Potent Carcinogens, Reproductive Toxicants, and Developmental Toxicants. Environ Sci Technol. 2023 May 2. doi: 10.1021/acs.est.2c07247. Epub ahead of print. PMID: 37129244.
- Swenberg JA, Moeller BC, Lu K, et al. Formaldehyde carcinogenicity research: 30 years and counting for mode of action, epidemiology, and cancer risk assessment. Toxicol Pathol. 2013;41(2):181-189.
- National Toxicology Program. Formaldehyde, Report on Carcinogens, Fifteenth Edition. Triangle Park, NC: National Institute of Environmental Health and Safety, 2021. Also available online.
- S. Environmental Protection Agency. Formaldehyde. Washington, DC: U.S. Environmental Protection Agency, 2013. Available online.
- https://www.lung.org/clean-air/at-home/indoor-air-pollutants
- Kanchongkittiphon W, Mendell MJ, Gaffin JM, et al. Indoor environmental exposures and exacerbation of asthma: an update to the 2000 review by the Institute of Medicine. Environ Health Perspect. 2015 Jan;123(1):6-20.
- Nazaroff WW, Weschler CJ. Cleaning Products and Air Fresheners: Exposure to Primary and Secondary Air Pollutants. Atmospheric Environment. 2004;38:2841-65.
- California Air Resources Board (CARB). Report to the California Legislature: Indoor Air Pollution in California. Sacramento, CA: California Environmental Protection Agency. 2005.
- Steinmann, AC. Fragranced Consumer Products and Undisclosed Ingredients. Environmental Impact Assessment Review 29,2009: 32-8.
- Zota AR, Aschengrau A, Rudel RA, Brody JG. Self-reported chemicals exposure, beliefs about disease causation, and risk of breast cancer in the Cape Cod Breast Cancer and Environment Study: a case-control study. Environ Health. 2010 Jul 20;9:40. doi: 10.1186/1476-069X-9-40.
- https://www.asbestos.com/asbestos/
- https://www.asbestos.com/asbestos/mesothelioma-researcher-sold-out-asbestos-giants/
- Spinazzè A, Campagnolo D, Cattaneo A, et al. Indoor gaseous air pollutants determinants in office buildings-The OFFICAIR project. Indoor Air. 2020 Jan;30(1):76-87.
- https://www.theguardian.com/us-news/2019/jun/25/lawmakers-concerned-chemicals-rubber-playgrounds-push-safety-rules
- Jacob SL, Cornell E, Kwa M, Funk WE, Xu S. Cosmetics and Cancer: Adverse Event Reports Submitted to the Food and Drug Administration. JNCI Cancer Spectr. 2018 Jun 20;2(2):pky012. doi: 10.1093/jncics/pky012.
- Faber S. The Toxic Twelve Chemicals and Contaminants in Cosmetics. https://www.ewg.org/the-toxic-twelve-chemicals-and-contaminants-in-cosmetics. May 5, 2020.
- Eberle CE, Sandler DP, Taylor KW, White AJ. Hair dye and chemical straightener use and breast cancer risk in a large US population of black and white women. Int J Cancer. 2020 Jul 15;147(2):383-391.
- Chang CJ, O’Brien KM, Keil AP, et al. Use of Straighteners and Other Hair Products and Incident Uterine Cancer. J Natl Cancer Inst. 2022 Dec 8;114(12):1636-1645.
- University of Chicago. General Social Survey Final Report. Trends in Psychological Well-Being, 1972-2014. April 2015.
- Geng S, Yang L, Cheng F, et al. Gut Microbiota Are Associated With Psychological Stress-Induced Defections in Intestinal and Blood-Brain Barriers. Front Microbiol. 2020 Jan 15;10:3067.
- Madison A, Kiecolt-Glaser JK. Stress, depression, diet, and the gut microbiota: human-bacteria interactions at the core of psychoneuroimmunology and nutrition. Curr Opin Behav Sci. 2019 Aug;28:105-110.
- Söderholm JD, Perdue MH. Stress and gastrointestinal tract. II. Stress and intestinal barrier function. Am J Physiol Gastrointest Liver Physiol. 2001 Jan;280(1):G7-G13.
- Saunderson EA, Spiers H, Mifsud KR, Gutierrez-Mecinas M, Trollope AF, Shaikh A, Mill J, Reul JM. Stress-induced gene expression and behavior are controlled by DNA methylation and methyl donor availability in the dentate gyrus. Proc Natl Acad Sci U S A. 2016 Apr 26;113(17):4830-5.
- Flati T, Gioiosa S, Chillemi G, Mele A, Oliverio A, Mannironi C, Rinaldi A, Castrignanò T. A gene expression atlas for different kinds of stress in the mouse brain. Sci Data. 2020 Dec 16;7(1):437.
- Secco D, Wang C, Shou H, Schultz MD, Chiarenza S, Nussaume L, Ecker JR, Whelan J, Lister R. Stress induced gene expression drives transient DNA methylation changes at adjacent repetitive elements. Elife. 2015 Jul 21;4:e09343. doi: 10.7554/eLife.09343. PMID: 26196146; PMCID: PMC4534844.
- Flores IE, Sierra-Fonseca JA, Davalos O, Saenz LA, Castellanos MM, Zavala JK, Gosselink KL. Stress alters the expression of cancer-related genes in the prostate. BMC Cancer. 2017 Sep 5;17(1):621. doi: 10.1186/s12885-017-3635-4. PMID: 28874141; PMCID: PMC5583991.
- O’Connor DB, Thayer JF, Vedhara K. Stress and Health: A Review of Psychobiological Processes. Annu Rev Psychol. 2021 Jan 4;72:663-688.
- Chida Y, Hamer M, Wardle J, Steptoe A. Do stress-related psychosocial factors contribute to cancer incidence and survival? Nature Clinical Practice Oncology 2008; 5(8):466–475.
- Yang T, Qiao Y, Xiang S, et al. Work stress and the risk of cancer: A meta-analysis of observational studies. International Journal of Cancer 2019; 144(10):2390–2400.
- Perego M, Tyurin VA, Tyurina YY, et al. Reactivation of dormant tumor cells by modified lipids derived from stress-activated neutrophils. Sci Transl Med. 2020 Dec 2;12(572):eabb5817. doi: 10.1126/scitranslmed. abb5817. PMID: 33268511; PMCID: PMC8085740.
- Moreno-Smith M, Lutgendorf SK, Sood AK. Impact of stress on cancer metastasis. Future Oncol. 2010 Dec;6(12):1863-81.
- Dai S, Mo Y, Wang Y, Xiang B, Liao Q, Zhou M, Li X, Li Y, Xiong W, Li G, Guo C, Zeng Z. Chronic Stress Promotes Cancer Development. Front Oncol. 2020 Aug 19;10:1492. doi: 10.3389/fonc.2020.01492.
- Mohan A, Huybrechts I, Michels N. Psychosocial stress and cancer risk: a narrative review. Eur J Cancer Prev. 2022 Nov 1;31(6):585-599.
- https://www.cdc.gov/media/releases/2017/p1116-fruit-vegetable-consumption.html#:~:text=Depending%20on%20their%20age%20and,of%20a%20healthy%20eating%20pattern.
- Mayer AB, Trenchard L, Rayns F. Historical changes in the mineral content of fruit and vegetables in the UK from 1940 to 2019: a concern for human nutrition and agriculture. Int J Food Sci Nutr. 2021 Oct 15:1-12.
- Davis DR, Epp MD, Riordan HD. Changes in USDA food composition data for 43 garden crops, 1950 to 1999. J Am Coll Nutr. 2004 Dec;23(6):669-82.
- Marles RJ. Mineral Nutrient Composition of Vegetables, Fruits and Grains: The Context of Reports of Apparent Historical Declines. Journal of Food Composition and Analysis. 2017;56:93-103.
- Wallace TC, McBurney M, Fulgoni VL, 3rd. Multivitamin/mineral supplement contribution to micronutrient intakes in the United States, 2007-2010. J Am Coll Nutr. 2014;33(2):94-102
- Tulchinsky, T.H. Micronutrient Deficiency Conditions: Global Health Issues. Public Health Rev 32, 243–255 (2010). https://doi.org/10.1007/BF03391600
- Johnson IT. Micronutrients and cancer. Proc Nutr Soc. 2004 Nov;63(4):587-95.
- Donaldson MS. Nutrition and cancer: a review of the evidence for an anti-cancer diet. Nutr J. 2004 Oct 20;3:19. doi: 10.1186/1475-2891-3-19.
- Hossain S, Beydoun MA, Beydoun HA, et al. Vitamin D and breast cancer: A systematic review and meta-analysis of observational studies. Clin Nutr ESPEN. 2019 Apr;30:170-184.
- Skrajnowska D, Bobrowska-Korczak B. Role of Zinc in Immune System and Anti-Cancer Defense Mechanisms. Nutrients. 2019 Sep 22;11(10):2273. doi: 10.3390/nu11102273. PMID: 31546724; PMCID: PMC6835436.
- Revuelta Iniesta R, Gerasimidis K, et al. Micronutrient status influences clinical outcomes of paediatric cancer patients during treatment: A prospective cohort study. Clin Nutr. 2021 May;40(5):2923-2935.
- Ganguly S, Srivastava R, Agarwala S, et al. Prevalence of micronutrient deficiency and its impact on the outcome of childhood cancer: A prospective cohort study. Clin Nutr. 2022 Jul;41(7):1501-1511.
- Ganguly S, Srivastava R, Agarwala S, et al. Prevalence of micronutrient deficiency and its impact on the outcome of childhood cancer: A prospective cohort study. Clin Nutr. 2022 Jul;41(7):1501-1511.
- Hodges RE, Minich DM. Modulation of Metabolic Detoxification Pathways Using Foods and Food-Derived Components: A Scientific Review with Clinical Application. J Nutr Metab. 2015;2015:760689. doi: 10.1155/2015/760689.
- Ames BN. DNA damage from micronutrient deficiencies is likely to be a major cause of cancer. Mutat Res. 2001 Apr 18;475(1-2):7-20. doi: 10.1016/s0027-5107(01)00070-7. PMID: 11295149.
- Ames BN, Wakimoto P. Are vitamin and mineral deficiencies a major cancer risk? Nat Rev Cancer. 2002 Sep;2(9):694-704.